JavaScript is required to view this application.
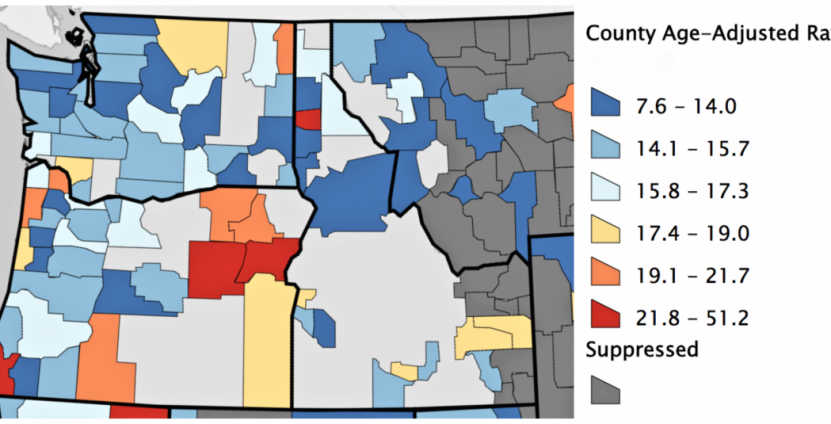
Making better decisions to prevent colon cancer